

SARS-COV-2 AND COVID-19
“My interview with the Microbiologist continues, dr. Sandra Mazzoli. The topic is the most discussed these days, the use of serological tests, for SARS-CoV-2 and the meaning of the detection of antibodies produced against the virus. Rapid tests can be of diagnostic help in selecting a population of positive or not positive subjects, to be started on the PCR test “. A.S.
Humoral immunity in the population: what we know and what we need to know; what we need to do.
by Sandra Mazzoli
Much has been done to deal with the new pandemic emergency COVID-19 in the Italian population and in the countries where the SARS-CoV-2 virus has occurred, also in consideration of the fact that very little time has passed, three months, from the report to the World Health Organization of the first cases at the end of December 2019 by the Chinese government. Never has a virus spread so quickly on the whole world.
Little is known, however, on the antibody-mediated humoral immunity produced during infection, in the infected population, in the “contacts” and in the asymptomatic and paucisymptomatic, both in high and low endemic areas.
The immune response against microorganisms is complex, it can be innate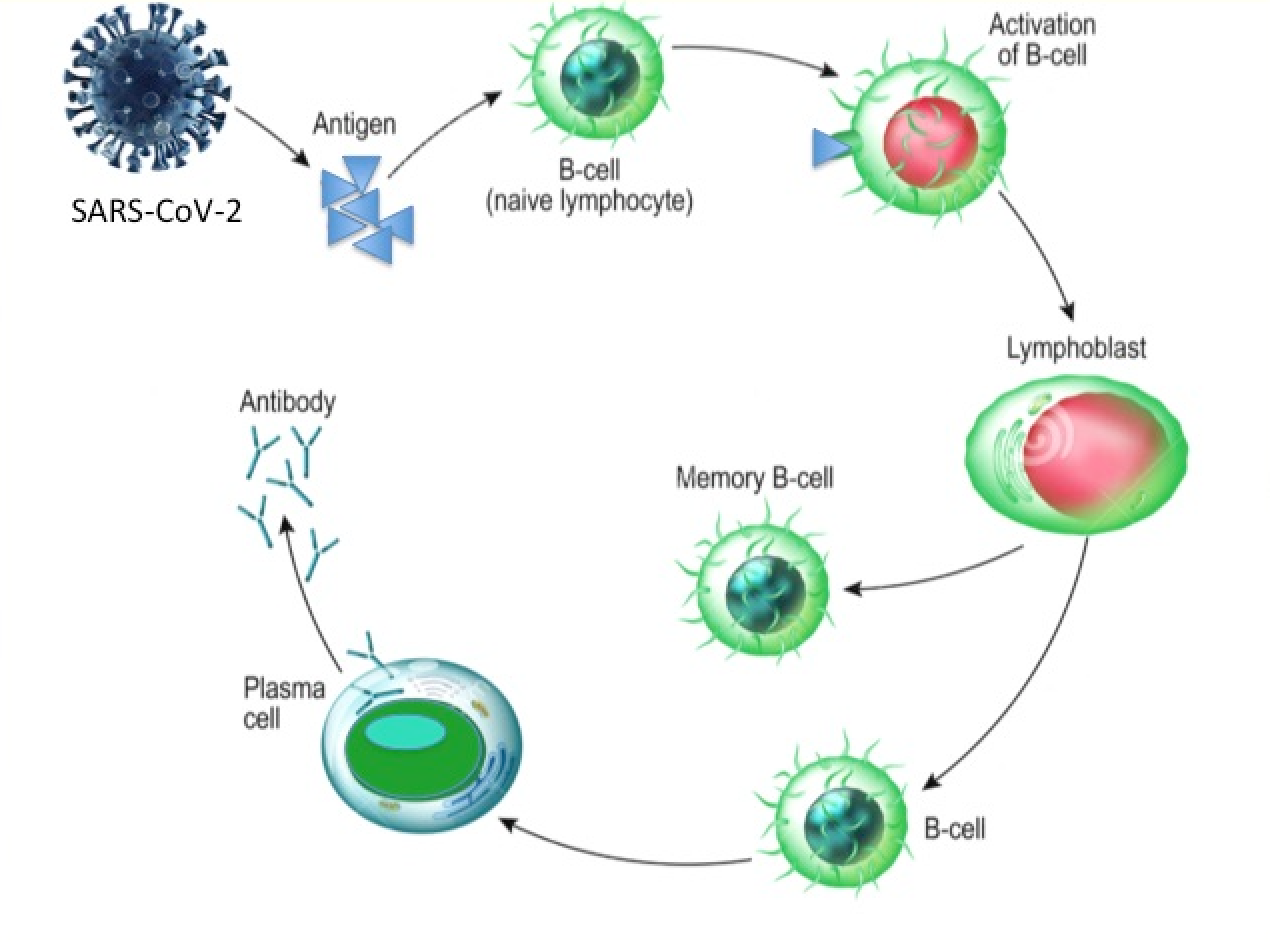 (NK cells, monocytes, granulocytes) and adaptive (T and B lymphocytes). B lymphocytes are responsible for the formation of antibodies which are of different classes: IgM, IgA, IgG in infections.
(NK cells, monocytes, granulocytes) and adaptive (T and B lymphocytes). B lymphocytes are responsible for the formation of antibodies which are of different classes: IgM, IgA, IgG in infections.
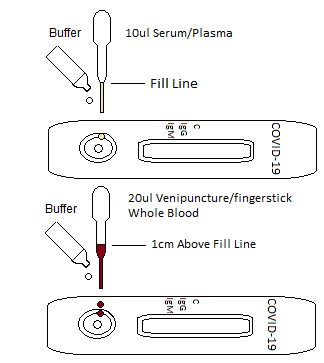
Since December 2019 various diagnostic tests have been developed also for the detection of specific antibodies against SARS-CoV-2, some of which are rapid, which are being talked about a lot these days, with good, some excellent, sensitivity (Ability to detect positives) and specificity (Ability to detect negatives). These tests are capable of detecting total antibodies and all individual specific antibody classes against SARS-CoV-2, i.e. IgG and IgM and IgA. Rapid ones usually detect IgM and IgG.
 Meaning of the antibody classes: IgM are considered the first antibodies that form in the immune response and are used to immediately try to neutralize the microorganism; IgA are also formed at the same time as IgM, they are also produced mainly in secretions and the first-line antibodies present on the mucous membranes are considered. When they persist for a long time in the blood, antibodies that mark chronic infection are considered. IgG are formed later, from the seventh day of infection onwards and are present in the convalescence phase and are those antibodies that usually help us in healing; thanks to the phenomenon of immune memory represent the class of antibodies that is formed when it comes in contact with the same microorganism again or after vaccinations, and they represent the so-called neutralizing antibodies, that is protective against infection. They are responsible for the “herd immunity” or better Group or Community.
Meaning of the antibody classes: IgM are considered the first antibodies that form in the immune response and are used to immediately try to neutralize the microorganism; IgA are also formed at the same time as IgM, they are also produced mainly in secretions and the first-line antibodies present on the mucous membranes are considered. When they persist for a long time in the blood, antibodies that mark chronic infection are considered. IgG are formed later, from the seventh day of infection onwards and are present in the convalescence phase and are those antibodies that usually help us in healing; thanks to the phenomenon of immune memory represent the class of antibodies that is formed when it comes in contact with the same microorganism again or after vaccinations, and they represent the so-called neutralizing antibodies, that is protective against infection. They are responsible for the “herd immunity” or better Group or Community.
To date, only two scientific papers have been published in this international SARS-CoV-2 infection in accredited international journals dealing with the presence of antibody in the population of infected or paucisymptomatic patients in China.
SARS-CoV-2 infection in accredited international journals dealing with the presence of antibody in the population of infected or paucisymptomatic patients in China.
The humoral immune response is documented in an early work by Guo et al., Published in Clinical Infectious Disease on March 21, 2020, which studied 82 confirmed COVID-19 cases and 58 probable suspected cases with negative PCR, but typical clinical manifestations; all three specific IgM, IgA and IgG antibody classes were searched. The antibodies of the IgM, IgA and IgG class were already present in the first days from the presentation of the symptoms and were already detectable by the fifth day of infection. During the acute phase, IgM and IgA were present in 85.4% and 92.7% of patients, respectively, with their concomitant presence already on the fifth day from the onset of symptoms. For IgG the average time of appearance was on the 15th day, they appeared in some patients from the first week and increased with an increase in production up to the plateu on the 21st day. Since the onset of symptoms, viral RNA PCR, positive in more than 90% of patients from 1-3 days, decreased to 80% on the 6th day and still dropped to 50% after the 14th day. The ability to diagnose COVID-19 (detection rate, DT) of PCR was higher than that of specific IgM until the 5th day after the advent of symptoms, after which the IgM was proved more efficient in demonstrating recent infection. Overall, for PCR, the “Detection rate” was 51.9% while, if the IgM test was added in the diagnosis of negative PCR, it rose significantly to 98.6% DT of the detection of the infection.
The work of Zhao and colleagues (Clinical Infectious Diseases, 2020, March 28) on 173 COVID-19 patients also shows that combining the search for IgG and IgM antibodies, even in the early stages of infection, increased the chances of diagnosis.
Furthermore, a high antibody titer in COVID-19 patients was associated with a worse clinical classification and more severe disease.
 Therefore, supporting the serological test for IgM increases the ability to find positive at the beginning of the infection, with a greater sensitivity if compared to the PCR test used alone. This data are particularly important in the initial stages of the pandemic, and of infection, when appropriate diagnostics, capable of detecting all true positives, allow to limit the spread of the virus. We are at that very moment, currently. Even in the presence of areas with a less extensive viral spread over the territory, using the IgM test (especially the rapid one) would allow to evaluate the small initial clusters of infection very well.
Therefore, supporting the serological test for IgM increases the ability to find positive at the beginning of the infection, with a greater sensitivity if compared to the PCR test used alone. This data are particularly important in the initial stages of the pandemic, and of infection, when appropriate diagnostics, capable of detecting all true positives, allow to limit the spread of the virus. We are at that very moment, currently. Even in the presence of areas with a less extensive viral spread over the territory, using the IgM test (especially the rapid one) would allow to evaluate the small initial clusters of infection very well.
The viral PCR / RNA, improperly called “Swab” according to the method of collection of biological material, although with a high analytical sensitivity, would no longer represent the “golden standard” (Wang M. et al; MedRxiv 2020 Feb. 18) since ‘the real world performance of the RNA test has proven unsatisfactory. In fact, the many variables that accompany the PCR test must be considered, the performance of which depends on factors such as the types of biological samples, the different stages of the infection, the methods of collection of the sample and the quality and characteristics of the test used and who is utilising it. Often the viral genome, especially in the initial stages of infection, is not present in sufficient quantity at the sample collection site, or has already disappeared from the upper respiratory tract, nasopharynx, and deep samples are not taken, from the lower respiratory tract , e.g. alveolar washes, or from the blood and from the oro-fecal tract (anal swab), all biological materials where the virus can be present and searched with biomolecular methods. An incorrect or poorly performed sampling of biological material (pharyngeal swab), can affect the result of the test which would be negative, causing the time window of viral replication and the consequent elimination of the virus in the environment to be lost.
collection of biological material, although with a high analytical sensitivity, would no longer represent the “golden standard” (Wang M. et al; MedRxiv 2020 Feb. 18) since ‘the real world performance of the RNA test has proven unsatisfactory. In fact, the many variables that accompany the PCR test must be considered, the performance of which depends on factors such as the types of biological samples, the different stages of the infection, the methods of collection of the sample and the quality and characteristics of the test used and who is utilising it. Often the viral genome, especially in the initial stages of infection, is not present in sufficient quantity at the sample collection site, or has already disappeared from the upper respiratory tract, nasopharynx, and deep samples are not taken, from the lower respiratory tract , e.g. alveolar washes, or from the blood and from the oro-fecal tract (anal swab), all biological materials where the virus can be present and searched with biomolecular methods. An incorrect or poorly performed sampling of biological material (pharyngeal swab), can affect the result of the test which would be negative, causing the time window of viral replication and the consequent elimination of the virus in the environment to be lost.
 Many “suspicious” patients must be tested multiple times for multiple days with multiple samples before confirming the diagnosis. In the COVID-19 patient this leads to a delay in early diagnosis and subsequent management of the patient with consequent risk for life, in the absence of suitable treatments and preventive quarantine (Zhao and colleagues, Clinical Infectious Diseases, 2020, March 28).
Many “suspicious” patients must be tested multiple times for multiple days with multiple samples before confirming the diagnosis. In the COVID-19 patient this leads to a delay in early diagnosis and subsequent management of the patient with consequent risk for life, in the absence of suitable treatments and preventive quarantine (Zhao and colleagues, Clinical Infectious Diseases, 2020, March 28).
It also determines the possibility for the “false negative” patient, or for the “asymptomatic individual”, always negative PCR, to become a viral super-diffuser, a super-spreader, hindering the efforts to contain the infection .
Furthermore, the easy-to-perform serological test can also be used in remote areas, where PCR tests cannot be performed.
It is important to underline how in both these studies carried out in China, and as already present in studies on SARS since the 2000s, in all patients there was an early seroconversion of IgM, IgA and IgG antibodies, i.e. at the very early stages of infection against both SARS-CoV-1 and SARS-CoV-2. The cumulative seroconversion curve for total antibodies (IgM, A, G) and IgM has reached 100% approximately one month after the advent of symptoms (Zhao and colleagues, Clinical Infectious Diseases, 2020, March 28). Critical and non-critical patients did not show significant differences for the three antibody markers. The authors also emphasize here how the combined use of RNA and antibody tests has markedly increased the sensitivity of the pathogenetic diagnosis of COVID-19. Another important point underlined by the Authors is that the increase in the production of antibodies during infection does not always coincide with the negative effect of viral RNA, especially in the most critical patients, suggesting the hypothesis that the production of antibodies is not sufficient to eliminate the virus. The amount of total antibodies produced in critically ill patients was significantly higher than in non-critically ill patients.
Age, gender and total antibody titre were independent factors associated with clinical classification based on severity.
The data discussed so far suggests that combining viral RNA and antibody tests significantly increases the sensitivity of detecting COVID-19 patients.
These data indicate serological tests as an important supplement to viral RNA during the course of the disease.
When can we then hypothesize to test antibodies? In what settings?
In the patient when a COVID-19 is suspected and the clinical signs are all there, but the viral RNA is negative; there a positive test for antibodies, especially if IgM or IgA are present, increases the possibility of making a diagnosis. Furthermore, in RNA positive patients, antibody seropositivity indicates the presence of induction of antibodies. If these are maintained over time and are protective, this is all to be evaluated, since the pandemic has erupted too recently. Subsequent epidemiological studies will tell us and antibody tests are suitable for carrying them out.
but the viral RNA is negative; there a positive test for antibodies, especially if IgM or IgA are present, increases the possibility of making a diagnosis. Furthermore, in RNA positive patients, antibody seropositivity indicates the presence of induction of antibodies. If these are maintained over time and are protective, this is all to be evaluated, since the pandemic has erupted too recently. Subsequent epidemiological studies will tell us and antibody tests are suitable for carrying them out.
In healthy contacts if in quarantine, if a positive antibody test is found, RNA tests should be monitored frequently and the contact contacts in turn should be monitored closely.
Asymptomatic seropositive individuals can be thought to be “asymptomatic diffusers” in the population.
Since it has been a short time since the SARS-CoV-2 infection occurred in the population, the total antibody positivity, all the antibody classes, according to some authors, can be considered in all respects as a marker of recent infection, like the single presence of IgM.
On the other hand, we have seen that all three antibody classes occur early, already, in many subjects, a week after the onset of the presentation of symptoms.
 In some COVID-19 patients, the amount of IgG produced seems very marked and their production would not represent a protection against the virus but rather a negative prognostic and severity marker of the infection. In fact, it has been proposed (Fu Y. Et al.; Virological Sinica 2020) that the aggravation of the disease would correlate with a secondary inflammatory response that would occur precisely when the neutralizing antibodies of the IgG class are formed against the viral S protein (Spike protein). These would not completely neutralize the virus, on the contrary, the immune virus- neutralizing antibody-complexes would attach to the cell receptor for complement-FCR on the cell, causing an increase in the inflammatory response and in the viral cell infection, with consequent further lung damage, as proven for SARS (Liu L. et Al.; 2019).
In some COVID-19 patients, the amount of IgG produced seems very marked and their production would not represent a protection against the virus but rather a negative prognostic and severity marker of the infection. In fact, it has been proposed (Fu Y. Et al.; Virological Sinica 2020) that the aggravation of the disease would correlate with a secondary inflammatory response that would occur precisely when the neutralizing antibodies of the IgG class are formed against the viral S protein (Spike protein). These would not completely neutralize the virus, on the contrary, the immune virus- neutralizing antibody-complexes would attach to the cell receptor for complement-FCR on the cell, causing an increase in the inflammatory response and in the viral cell infection, with consequent further lung damage, as proven for SARS (Liu L. et Al.; 2019).
However, serology tests that show specific antibodies to SARS-CoV-2 have an important diagnostic value that would allow us now, in this initial moment of the pandemic epidemic
- to identify additional COVID-19 positive patients;
- to recognize patients at risk of severe infection;
- to improve their clinical management,
- to monitor the effectiveness of therapies;
- to follow the symptomatic and asymptomatic “contacts”,
- to identify the asymptomatic “spreader”, so important in the spread of the virus in the population;
- to follow the healed and assess the presence of immunity from “relapse” or from “reinfection” possibly permanent;
- to evaluate the prevalence of the virus in the population or in groups of subjects at risk,
- to always choose better diagnostic techniques based on the prevalence of the virus in the population
- to implement targeted preventive and containment measures.
Finally, the serological tests will represent a sure reference test to evaluate the presence of protective antibodies in the population after vaccination.
In simple words, however, at the moment, having positive antibodies in serological tests would not mean that the infectious phase of the infection has passed or, even, that you are protected.
Studies will be needed to understand if the antibodies produced after the infection are neutralizing the virus and stable over time, thus protective.
In these days we can see the possibility of carrying out rapid IgM and IgG tests, available in accredited laboratories and also purchasable by private individuals. Obviously, safe and validated tests.
Personally, for the reasons expressed so far, being all of us in an emergency situation, I consider important to do them and repeat them after 15-20 days, to understand how many of us have the infection in progress or / and are unconscious spreaders of the virus, in order to provide for a narrower containment and the possibility of carrying out the detection of viral RNA as well. If this turns out to be positive, it would also allow people to undergo proper clinical and diagnostic follow-up.
All with a view to containing a new, pandemic and lethal infection.
Sandra Mazzoli

